
Long pauses in breathing, gasping for air, the jarring “goose honk” noise coming from your little one… sound familiar? Goodness, I do not miss those days.
I still remember the guilt I felt realizing that somewhere along the way, my daughter had paused her breathing, only for me to suddenly hear a terrifying squeaky gasp for air as her body jolted upright in fear. The constant stridor while she slept. The choking during bottles and forgetting to breathe. Unzipping her onesie repeatedly to check for retractions and see how severe they were. It was all incredibly scary.
So mama, if this is what you are going through right now, my heart truly goes out to you. I’m hopeful that sharing our story may help you troubleshoot possible next steps and feel a little less alone.
My husband and I noticed our daughter’s squeaky breathing shortly after bringing her home from the hospital. Before long, we realized she was having pauses in her breathing followed by these large squeaky gasps for air, almost as if she had forgotten to breathe for a moment. She would throw her whole body upward, sometimes startling herself awake and crying afterward.
We also noticed retractions, which is the pulling in of the skin during breathing. These can sometimes be seen around the ribs, diaphragm area, or throat, the latter often referred to as a tracheal tug.
From our early research, we came across something called laryngomalacia and brought our concerns to her pediatrician, who agreed it was a possibility.
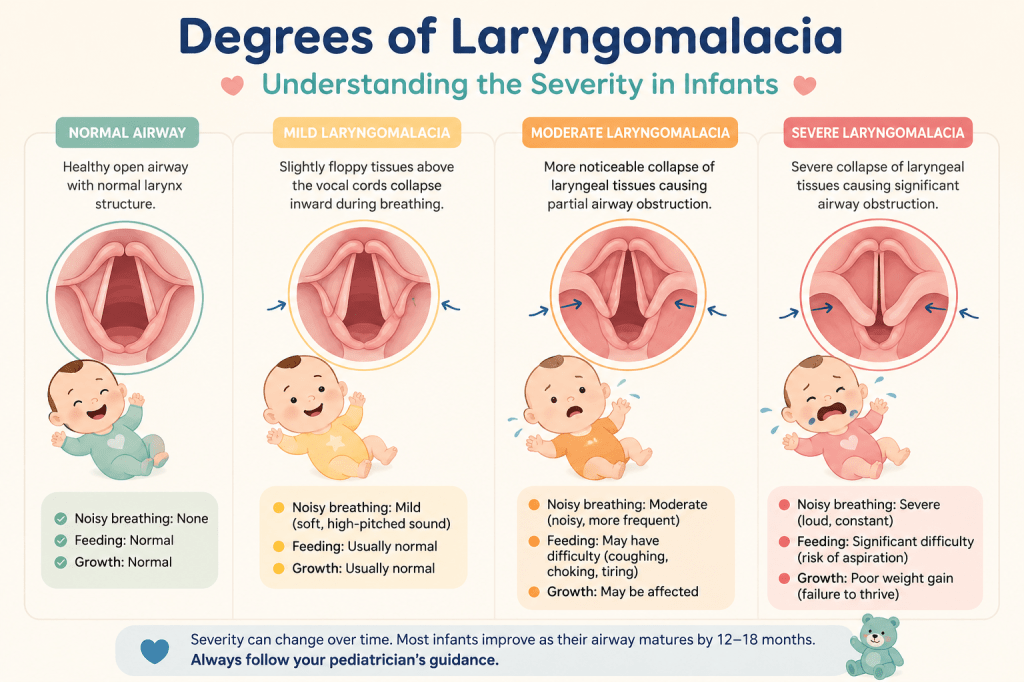
Laryngomalacia is a condition in infants where the tissues above the vocal cords are softer and floppier than usual. During breathing, these tissues can temporarily fall inward, partially blocking the airway and causing noisy breathing, often described as a high-pitched sound called stridor. Symptoms are commonly more noticeable during feeding, crying, reflux episodes, excitement, or while lying flat on the back. In many cases, laryngomalacia improves as a baby grows and the airway structures become stronger.
However, because of the severity of some of our daughter’s symptoms, we wanted to rule out a more severe case, especially after learning that some infants may require surgical intervention.
We requested a referral to an ENT because, honestly, it sounded terrifying. Had we not already learned about laryngomalacia, we likely would have taken her to the emergency department during many of those episodes. It was that alarming to witness as a parent.
We ultimately brought her to a highly reputable children’s hospital in Boston for an ENT consultation, where they briefly used a small scope through her nose to visualize her airway and voice box area. She left with a diagnosis of moderate laryngomalacia, along with orders for a swallow study and chest X-ray.
The advice? Time.
Honestly, this was one of the most frustrating responses we repeatedly heard throughout so many aspects of our daughter’s medical journey. However, I will say this was one diagnosis where the specialists were ultimately spot on. As she grew, her symptoms gradually improved, and by around six months old, she was clear of symptoms.
Phewf!
Please see below for a list of common symptoms and possible next steps.
- Noisy breathing (often a high-pitched sound called stridor)
- Symptoms worsening while lying on the back
- Noisy breathing during feeding, crying, excitement, or reflux episodes
- Retractions (skin pulling in around the ribs, neck, or chest while breathing)
- Tracheal tugging
- Congestion or “wet” sounding breathing
- Feeding difficulties
- Choking, coughing, or sputtering during feeds
- Frequent spit-up or reflux symptoms
- Slow feeding or tiring during feeds
- Difficulty coordinating sucking, swallowing, and breathing
- Gasping episodes
- Poor sleep due to discomfort or breathing noise
- Poor weight gain in more severe cases
- Cyanosis (bluish discoloration) in severe cases
- Apnea/breath-holding episodes in more severe cases
What next?
If you strongly suspect your child may have laryngomalacia, I would recommend discussing your concerns with your pediatrician and asking whether a referral to a pediatric ENT would be appropriate.
While some pediatricians may feel confident identifying likely laryngomalacia based on symptoms and clinical presentation, a pediatric ENT is typically able to more closely evaluate the airway structure and determine the severity of the condition. Understanding whether your child’s case is considered mild, moderate, or severe can be extremely helpful in guiding next steps and monitoring.
If possible, I personally found it reassuring to seek care through a pediatric ENT affiliated with a children’s hospital, especially because these specialists evaluate infant airway conditions regularly.
One thing that helped me tremendously throughout this journey was connecting with other parents going through similar experiences. I have always found support groups on Facebook to be incredibly helpful. If you tend to be on the shyer side, Facebook does offer an anonymous posting option within many groups that hides your name and profile information.
Lastly, if you leave an appointment still feeling uneasy or unheard, do not hesitate to seek a second opinion — even from another pediatric ENT within the same hospital system. Trust your instincts as a parent. You know your child best. You got this mama.
Recommended Facebook support group: Laryngomalacia Support Group

